 |
| MERLOT
Journal of Online Learning and Teaching |
Vol. 3,
No. 3, September 2007
|
|
|
|
Developing a Public
Health Web Game to Complement Traditional
Education
Methods in the Classroom
Eileen O’Connor
School of Human Kinetics
Faculty of Health Sciences, University of Ottawa
Ottawa, ON CA
Karen Phillips
Health Sciences Program
Faculty of Health Sciences, University of Ottawa
Ottawa, ON CA
|
|
ABSTRACT
Infectious disease outbreaks, whether natural or deliberate,
constitute a growing health concern. The impending
reality of this situation is indicative of the
exigency in which the government recently created
the Canadian Public Health Agency. As with other
countries, Canada is committed to enhance its
capacity to respond to emergencies through increased
investment in the interdisciplinary training of
medical and public health professionals. This
article describes our initiative to create an
innovative scenario-based web game of an infectious
disease outbreak to be used in medical and public
health university-level courses. By providing
real-life, concrete examples of health crisis
situations, students will develop strong
critical-thinking skills while examining the cause
and effect relationship of actions. Ultimately, our
goal is to transfer current knowledge on best
practices in emergency preparedness to
university-level students.
KEYWORDS:
Emergency management, epidemics, goal-based
scenarios, infectious disease, public health,
simulation, game, students, training, online
education
|
|
INTRODUCTION
Infectious disease outbreaks, whether natural or
deliberate, constitute a growing health concern.
Recent terrorist attacks in London and Madrid, or
the natural disasters in Peru, the Hurricane Katrina
in the US Golf Coast, the Tsunami in Indonesia, or
disease outbreaks like the 2003 SARS outbreak in
Toronto, all highlight the need for better training,
communication, integration and improved emergency
responsiveness. Health care workers, researchers,
and policy advisors recognize the need for enhanced
collaborative and coordinated communications and
training for healthcare workers as ‘first
responders’. There is also a need to establish
better training guidelines and raise public
awareness of how to manage and contain infectious
diseases. Thus, the genesis of this project stems
from the need to engage and train future healthcare
workers, health policy analysts and first responders
to respond to an infectious disease outbreak. Our
public health scenario-based game, OUTBREAK!
serves to fill this gap by offering students the
chance to role play and test their abilities in
understanding, mitigating and managing an infectious
disease outbreak in a large urban city.
This paper discusses the developmental stage of
developing the game prototype for OUTBREAK!
Future phases in this game development include the
testing, evaluation and subsequent revision of the
prototype once it has been tested in a
computer-equipped undergraduate health sciences lab
classroom.
Design Strategy
Training health care specialists through e-learning strategies and
role-playing games has proven to be widely
successful. As Garris,
Ahlers and Driskell (2002) contend, these
games are both engaging
and instructive in their design, with students
demonstrating a high retention of new material
acquired. In the Canadian context, there are
few public health web-based scenario games
developed, thereby providing a substantial niche for
our scenario-based game.
As an interactive and visual tool, OUTBREAK! is designed to engage
students whose learning styles are best served
though the use of concrete examples and role playing
experiences (Garris et al., 2002).
The game is intended for small groups to play in
order to emphasize a team-based approach, and to
draw on the range of student’s different areas of
knowledge and expertise.
Development of an effective, interactive game
required two phases. Phase I focused on the
characterization of educational objectives to ensure
that the game would sufficiently address
disciplinary content, provide for consequential
decision-making and enable students to learn through
success and failures. This phase consisted of
setting learning objectives, (disciplinary expertise
and necessary preparation required to play the
game), the target audience (identification of game
end-users), and characterization of the infectious
disease underlying the game. Phase II consisted of
determining the conceptual framework including the
game design, objectives, scenario design (setting,
context, roles and responsibilities of key
decision-makers), consequential decision-making and
learning uptake (identification of parameters for
success and failure, debriefing and learning
assessment). The scenario development design was
facilitated by a rigorous consultative process with
experts in infectious disease management, public
safety, computer software design, e-learning,
education curriculum design and/or effective
classroom teaching. As undergraduate students are
the end-users of this game, it will be essential to
incorporate student participation and feedback
during the design phases of the scenario.
Infectious Disease Agent
A critical first step in design development was to determine the nature
of the health emergency. To ensure an integrated
co-operative response from various sectors (health
care, government, public health agency), we selected
an infectious disease agent that could rapidly be
transmitted from person to person, with marked
symptoms and complications including mortality.
Literature reviews were conducted to identify the
most appropriate infectious disease agent and best
practices for diagnosis, treatment and public
response.
The biological agent responsible for our simulated infectious disease
outbreak is modeled after a norovirus. Norwalk-like
viruses or ‘nor viruses’ are a leading cause of
acute gastroenteritis epidemics in industrialized
countries (Moe, Christmas, Echols and Miller, 2001).
Norovirus outbreaks are characterized by symptoms of
severe vomiting, watery diarrhea, nausea, abdominal
cramps, fever and general malaise. Onset of symptoms
is generally 15-48 hours after exposure with illness
lasting 12-60 hours (Hutson, Atma and Estes, 2004).
Noroviruses are the cause of acute gastroenteritis
in people of all ages with documented transmission
following direct person-to-person contact,
consumption of contaminated food, namely raw
oysters, bakery products, fresh fruit and
vegetables, (Berg, Kohn, Farley and McFarland, 2000;
Long, Adak, O’Brien and Gillespie, 2002;) water
(ice, well or bottled water, and during swimming,
(Cannon et al., 1991; Pedalino et al., 2003;) and
following exposure to contaminated environmental
surfaces and to airborne droplets containing the
virus (Marks et al., 2003). Noroviruses are
transmitted very easily due in part to their low
infectious dose with less than 10 virions sufficient
to infect a healthy adult (Moe et al., 2004). In
our web game OUTBREAK!, contamination of a
fictitious brand of bottled spring water (Corneil’s
Best) with a variant strain of Norwalk virus was
selected as the source of the foodborne/waterborne
outbreak.
Learning Objectives and Pedogogical Approach
Learning objectives were identified in five major
categories (Table 1):
1. Observation and analysis: The first learning
objective requires users to analyze descriptive
health sciences scenarios, comprised of both text
and graphics. Information provided early in the
learning exercise must be retained for successful
problem assessment and derivation of solutions
throughout the game (Schank, Fano, Bell and Jona,
1993).
2. Knowledge application - Learning through failure
and success: Users must use knowledge acquired
through a wide range of courses to understand
scenario descriptions that include use of medical
terminology, scientific language and scientific
approaches (Schank et al., 1993).
3. Health science expertise - Problem-based
learning: As this scenario-based game was designed
for interdisciplinary health sciences programs, it
was essential for the game to provide a greater
understanding of health sciences theory and
approaches, particularly in the fields of anatomy,
physiology, epidemiology and public health. (Schank
et al.).
4. Risk communication- reflection opportunities: An
integral part of any organizational response to
public health crises is effective and timely risk
communication. Decisions regarding when to release
information on sensitive public health and safety
issues, how to select the individual delivering the
messages and when to involve the media are complex
and critical management skills that will be
addressed in the game design (Schank et al.).
5. Crisis-management, consequential decision-making,
goal based scenario: Consequences of decisions
regarding the triage of emergency room patients,
communications with public health authorities,
strategic deployment of emergency personnel and
resources will illustrate the complex and dynamic
interrelationships between emergency personnel,
their communications and access to specialized
equipment and protection (Schank et al.).
Table 1. Learning objectives and pedagogical
approach used to develop scenario-based game
design.
|
ormal" style="text-align:justify">
Pedagogical Approach
(Shank, 1993) |
|
Observation and analysis |
Assessment through replaying events |
|
Knowledge application |
Learning through failure and success |
|
Health sciences expertise |
Problem-based learning |
|
Risk communication |
Reflection opportunities |
|
Crisis management, consequential decision-making |
Goal based scenarios |
Game Objective
The objective of this public health scenario-based game, OUTBREAK!,
is to successfully mitigate and manage the
infectious disease outbreak. Containment of the
outbreak will be measured by the absence of new
cases of infection, and minimal number of
casualties. Effective management of the outbreak
will be measured by minimal disruption in the
operation of the game city services including
maintaining a strong economy, tourism and special
events.
Game Framework and Design
The fundamental objective of OUTBREAK! is to enable students to
make informed decisions within the context of an
infectious disease health emergency. Decisions will
be required at three levels or ‘lenses’: 1.
Municipal government, 2. Public health and 3.
Health care (Figure 1). The game
requires players to make a series of decisions based
on six situations that occur within the linear
timescale of an infectious disease outbreak (Figure
2). OUTBREAK! is divided into six levels,
each level requiring students to answer four
questions within one of the three lenses (municipal
government, public health, healthcare; Figure 1). By
dividing the game into different levels, players are
required to demonstrate a level of expertise within
each lens in order to progress to the next level.
This will further the educational objectives by
ensuring that all students gain exposure to each of
the three lenses.
A decision-matrix (Table 2) will be used
to stream students through to the next situation on
the subsequent level. For each situation, players
must make decisions for four scenarios. Each
scenario presents the players with four possible
options (Table 3) representing one Good decision,
two Neutral decisions and one Bad decision. Each
question will depict an event during the timeline of
an infectious disease outbreak (scenario). Scenarios
will be introduced in a Scenario Context page which
will provide the setting of the event, the
decision-maker’s profile and information necessary
to provide context to the event. Finally, a Scenario
Feedback page will provide the player with specific
feedback regarding the decision selected
(Figure 3). Players
that consistently select Good decisions are directed
through the decision tree thereby maximizing total
score (Figure 2). The rationale underlying this
strategy is twofold. First, pedagogically, it was
important to design a decision tree that would
enable players to overcome bad decisions by making
good decisions in subsequent situations. Second, as
individuals often make decisions that are not
intrinsically harmful or disadvantageous, it was
decided that 50% of the options would represent
neutral decisions. These neutral decisions would
require players to make sound decisions that would
fall within the limits of best practice. The
decision score matrix (Table 3) is used to determine
how each decision cluster (representing a single
level) contributes to the decision path for the next
scenario situation.
|
| |
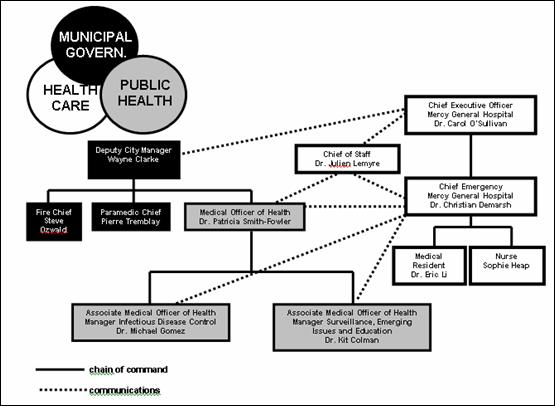
Figure 1. Decision-Makers Map.
|
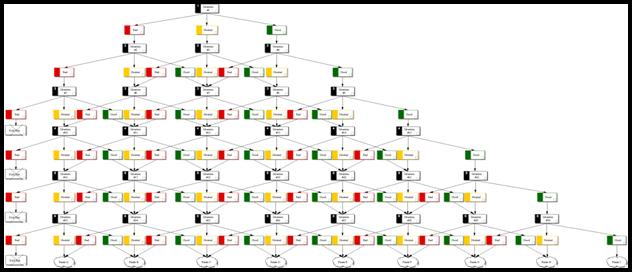
Figure 2A. Full decision making tree. See
Fig. 2B for details.
|
|
|
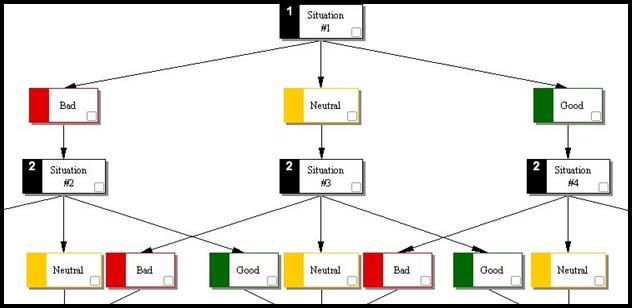
Figure 2B. Decision Tree details.
|
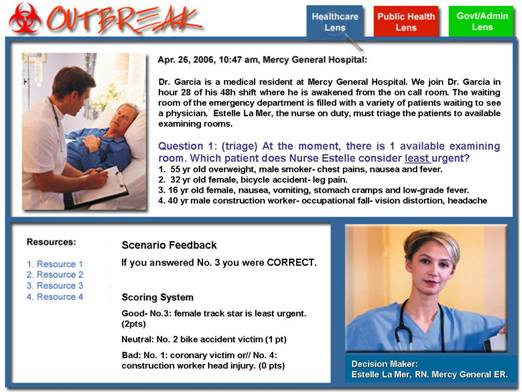
Figure 3. Scenario Design.
|
Table
2. Decision Score Matrix.
|
Choices |
Weighting |
Sample |
Score |
Feedback |
|
Decision 1A |
2 |
|
2 |
Good answer |
|
Decision 1B |
1 |
|
|
|
|
Decision 1C |
1 |
|
|
|
|
Decision 1D |
0 |
|
|
|
|
Decision 2A |
0 |
|
|
|
|
Decision 2B |
1 |
|
1 |
Neutral answer |
|
Decision 2C |
2 |
|
|
|
|
Decision 2D |
1 |
|
|
|
|
Decision 3A |
1 |
|
|
|
|
Decision 3B |
1 |
|
1 |
Neutral answer |
|
Decision 3C |
2 |
|
|
|
|
Decision 3D |
0 |
|
|
|
|
Decision 4A |
0 |
|
|
|
|
Decision 4B |
1 |
|
|
|
|
Decision 4C |
1 |
|
|
|
|
Decision 4D |
2 |
|
2 |
Good answer |
Table 3. Pedagogical Impact of Decision Score
Matrix.
|
Decision 1 |
Decision 2 |
Decision 3 |
Decision 4 |
Sum (Score%) |
Path |
|
Good (2) |
Good (2) |
Good (2) |
Good (2) |
8 (100%) |
GOOD |
|
Good (2) |
Good (2) |
Good (2) |
Neutral (1) |
7 (87.5%) |
GOOD |
|
Good (2) |
Good (2) |
Neutral (1) |
Neutral (1) |
6 (75%) |
GOOD |
|
Good (2) |
Good (2) |
Good (2) |
Bad (0) |
6 (75%) |
GOOD |
|
Good (2) |
Neutral (1) |
Neutral (1) |
Neutral (1) |
5 (62.5%) |
NEUTRAL |
|
Good (2) |
Good (2) |
Neutral (1) |
Bad (0) |
5 (62.5%) |
NEUTRAL |
|
Good (2) |
Good (2) |
Bad (0) |
Bad (0) |
4 (50%) |
NEUTRAL |
|
Good (2) |
Neutral (1) |
Neutral (1) |
Bad (0) |
4 (50%) |
NEUTRAL |
|
Neutral (1) |
Neutral (1) |
Neutral (1) |
Neutral (1) |
4 (50%) |
NEUTRAL |
|
Good (2) |
Neutral (1) |
Bad (0) |
Bad (0) |
3 (37.5%) |
NEUTRAL |
|
Neutral (1) |
Neutral (1) |
Neutral (1) |
Bad (0) |
3 (37.5%) |
NEUTRAL |
|
Good (2) |
Bad (0) |
Bad (0) |
Bad (0) |
2 (25%) |
BAD |
|
Neutral (1) |
Neutral (1) |
Bad (0) |
Bad (0) |
2 (25%) |
BAD |
|
Neutral (1) |
Bad (0) |
Bad (0) |
Bad (0) |
1 (12.5%) |
BAD |
|
Bad (0) |
Bad (0) |
Bad (0) |
Bad (0) |
0 |
BAD |
Learning Assessment
By limiting the game design to pre-determined options, this educational
tool will emphasize decision-making approaches
guided by consequences, penalties and rewards. The
individual weighting of each decision ensures that
game remains strategic, with only 27% of possible
options leading to the Good Path, 47% options
leading to the Neutral Path and 27% options leading
to the Bad Path. The strategic weighting of each
decision ensures that approximately 73% of possible
answers will propel the student through the game. If
a student makes a series of consecutive Bad
decisions, the game is over (Figure 2).
Performance in the game will be measured through a morbidity/mortality
score, which will be correlated to a ‘public health
expert scale’ (Table 4) ascertained using a disease
algorithm based on the amount of time the user takes
to complete decisions. Time penalties will be
awarded when players make Bad or Neutral decisions.
Strategic application of time penalties may also be
imposed for decisions that are considered critical
for successful resolution of the outbreak.
Table 4. Performance: Level of Public Health
Expertise.
|
Level 1 |
Public Health Expert (case range x-xx) |
|
Level 2 |
Public Health Associate (case range xx-xxx) |
|
Level 3 |
Public Health Novice (case range xxx-xxxx) |
|
Level 4 |
The Contaminator (case range >xxxx) |
Conclusion
The potential for OUTBREAK! to contribute to public health
education and training is significant. The selection
of a waterborne illness as the infectious disease
agent engages Canadian students with the parallels
to the 2000 Walkerton,
Ontario outbreak, which produced serious illness in
an estimated 2,300 people following exposure to E.
coli O157:H7- contaminated drinking water (Schuster
et al., 2005
). Since waterborne disease agents are responsible for some
of the largest disease outbreaks and public health
emergencies, inquiries into the cause of these
outbreaks have led to changes in public policy, and
increased awareness of the importance of
interagency/intragovernmental communication and
cooperation. Hence, creating a game around the
premise of a waterborne infectious disease outbreak
complements traditional teaching methods in
emergency preparedness by
providing an excellent case study for students to
learn more about healthcare response, health policy,
and disease management in emergency situations.
ACKNOWLEDGEMENTS:
We wish to thank the anonymous reviewers and the
journal editors for their excellent comments and
suggestions. We would like to recognize the
financial support from the Institute of Population
Health, and the Center for University Teaching at
the University of Ottawa for grants which permitted
the development of this game prototype. We also
thank several scientists at the Institute of
Population Health, including Wayne Corneil, Dr.
Carol Amaratunga and Dr. Louise Lemyre; the Center
for E-learning, TLSS, at the University of Ottawa,
including Richard Pinet, André Seguin, Rémi Rousseau
and Nicolas Hessler, and to our excellent student
research assistants, Hany Rizk, Naim R. El-Far, Alex
deMarsh and
Zainab Khan.
References
Berg, D.E., Kohn, M.A., Farley, T.A. & McFarland,
L.M. (2000).
Multi-state outbreaks of acute gastroenteritis traced to
fecal-contaminated oysters harvested in Louisiana.
Journal of Infectious Diseases. May;181 Suppl
2:S381-6. Review.
Cannon, R.O., Poliner, J.R., Hirschhorn, R.B., Rodeheaver, D.C.,
Silverman, P.R., Brown, E.A., Talbot, G.H., Stine,
S.E., Monroe, S.S. & Dennis, D.T. (1991). A
multistate outbreak of Norwalk virus gastroenteritis
associated with consumption of commercial ice.
Journal of Infectious Diseases, 164(5):860-3.
Garris,
R., Rober A.
&
James, E. D. (2002). Games, motivation and learning:
a research and practice model. Simulation
& Gaming,
Vol 33(4): 441-467.
Hutson, A.M., Atmar, R.L. & Estes, M.K. (2004). Norovirus disease:
changing epidemiology and host susceptibility
factors. Trends in Microbiology, Jun;12(6):279-87.
Long, S.M., Adak, G.K., O'Brien, S.J. & Gillespie, I.A. (2002). General
outbreaks of infectious intestinal disease linked
bottom:4.3pt;
margin-left:0in;text-align:justify">
Marks, P.J., Vipond, I.B., Regan, F.M., Wedgwood, K., Fey, R.E. & Caul,
E.O. (2003). A school outbreak of Norwalk-like
virus: evidence for airborne transmission.
Epidemiology and Infection, Aug;131(1):727-36.
Moe, C.L., Christmas, W.A., Echols, L.J. & Miller, S.E. (2001). Outbreaks
of acute gastroenteritis associated with
Norwalk-like viruses in campus settings. Journal
of American College Health, Sep;50(2):57-66.
Pedalino, B., Feely, E., McKeown, P., Foley, B., Smyth, B. & Moren, A.
(2003). An outbreak of Norwalk-like viral
gastroenteritis in holidaymakers travelling to
Andorra, January-February 2002. Euro
Surveillance. Jan;8(1):1-8.
Schank, R., Fano, A., Bell, B. & Jona, M.(1993). The design of goal-based
scenarios. Journal for the Learning Sciences,
3(4): 305-345.
Schuster, C. J., Ellis, A. G., Robertson, W. J.,
Charron, D. F., Aramini, J. J., Marshall, B. J. &
Medeiros, D.T. (2005). Infectious disease outbreaks
related to drinking water in Canada, 1974-2001.
Canadian Journal of Public Health, 96(4),
254-258.
|
|
|
|
|