Development of an Interactive Online Module to Prepare Students for Learning
to Measure Joint Range of Motion
|
Nicola Massy-Westropp, Susan Gilbert Hunt, Shylie Mackintosh, and Michael Lewis
School of Health Sciences
University of South Australia
East Campus, North Terrace
Adelaide, South Australia, AU 5000
nicola.massy-westropp@unisa.edu.au
Abstract
Within the University of South Australia, human anatomy is taught in many allied health undergraduate programs. One aspect of the course is developing student ability to measure joint range of motion (ROM) using a protractor like device called a goniometer. This is an important quantitative assessment, used frequently in the clinical setting. However, teaching staff struggle to provide individual feedback to each student or teach the theory and skill at a pace that suits each student. Anatomy teaching staff at the university developed and trialled an online joint ROM pre-class preparation module to allow students to learn the theory behind the skill, and then to see the assessment in class. The interactive module used brief text and images, followed by a self test. Students were then invited to use a virtual goniometer with a movie, their efforts accompanied by corrective feedback. Pre and post module questionnaires evaluating student satisfaction, level of knowledge and confidence were conducted and results were compared and analysed through content analysis and frequency of response. Overall results demonstrated voluntary student engagement and enjoyment, increased student understanding on joint ROM, and appreciation of the immediate feedback provided. The module has the potential to be embedded into the other courses or as revision before clinical placements.
Keywords: interactive tutorial; range of motion; goniometry |
Introduction
The knowledge and application of human anatomy is fundamental to most undergraduate health programs. Over the past twenty years, the teaching of anatomy has undergone significant changes with a move to greater use of web-based or computer-assisted learning. There is now less emphasis on dissection for students to learn anatomy (Brenton et al., 2007). Anatomy is a compulsory subject taught to large groups of students in the first undergraduate year of any health-related programme (O’Byrne, Patry & Carnegie, 2008). Although many students are overwhelmed by the new terminology and volume of information, students are asked to apply their anatomy knowledge immediately when learning how to measure joint range of motion (ROM).
Knowledge of anatomical landmarks is required in order to accurately measure ROM, which is one aspect of anatomy knowledge application common across a number of allied health professions. Range of motion is a measurement of how far a joint can be moved in one direction. Measurement of joint ROM involves the use of a goniometer (a protractor like device), the axis of which is placed on anatomical landmarks that correlate with the axis of the joint. The goniometer’s two arms are placed on the bones proximal and distal to the joint being measured and the measurement is then taken.ROM is recorded as a number of degrees, followed by the joint that has moved and the direction of the movement, for example, Mr B. has 75 degrees of wrist extension.
Measurement of joint ROM requires knowledge of anatomical landmarks surrounding the joints, comprehension of the terms that describe motion and understanding of the normal arc of motion of the joint being measured. Moreover, the person measuring the joint ROM has to know how to accurately position the goniometer and clearly instruct the client on the required movement. Within the clinical setting, ROM measurements allow health professionals to establish baseline information about a client’s joint movement, which can then be compared with normative data. Subsequent changes in movement resulting from therapy intervention can then be compared with baseline data. This also assists with the evaluation of ROM therapy interventions and the planning of further treatment. ROM measurements are also communicated with other health professionals treating the client, facilitating consistency in treatment.
Therefore, measurement of ROM is a fundamental skill that occupational therapists, physiotherapists, radiographers, physical trainers and podiatrists are taught as undergraduates at the University of South Australia. A number of processes have been employed from Scott (1993) to assist students to learn this practical skill, including learning the underlying theory, watching the skill being demonstrated and trying out the new skill both with supervision and independently. However, the teaching of anatomy within the university is also undergoing similar challenges to those discussed at the beginning of the paper. Furthermore, providing sufficient opportunity for students to observe and try practical skills in the classroom is often limited by the size of classes and reduced time for any face to face teaching activity. As a consequence, there are often time pressures and limited opportunity for students to practice and consolidate their skills in measuring joint ROM. Another issue for some students is that demonstrating the developing skill in front of peers can be anxiety provoking and this can limit their participation and learning. Moreover, it is impossible for the educator to provide feedback on all the activity in the classroom and students may develop incorrect estimates of their ability.
With the aim to overcome some of these challenges, anatomy teaching staff at the university worked together to develop and trial an online pre-class preparation ROM module, which allowed students to learn at their own pace and to develop a level of confidence with the skill prior to being observed by peers and a educator. The module also aimed to optimize time available in the practical class to consolidate skill development.
Literature Survey
Medline, CINAHL, Embase, and Google Scholar were searched without time or language limits, using key words; computer, online, web-based, range of motion, goniomet*, teaching, learning, surface anatomy. No published literature about online teaching of ROM was found, however an online learning environment was considered appropriate for learning the principles of ROM, as recent research indicates that students find online resources motivating when learning anatomy (Jastrow & Hollinderbaumer, 2004). There is also research to indicate that an online learning resources result in students performing better in relation to learning anatomical landmarks (Hallgren, Parkhurst, Monson & Crewe, 2002). These online contexts have also been found to support students develop of self-regulatory processes in learning when there is direct feedback (Azevedo, 2007). Moreover, such resources can allow students to progress at their own rate, repeat aspects of their preparation and can assist with preparation for practical class or assessment ( Chickerin & Gamson 1987). The development, trial and evaluation of this module will be further discussed in this paper.
Methods
Online learning tool
The ROM module was designed and developed with the support of a teaching and learning grant from the University of South Australia. Ethical committee approval from the University of South Australia. was also obtained to allow evaluation of the module.
The ROM module was designed with the elements of a computer game, in that it had goals, it was interactive and it had rewards in the form of immediate feedback on answers (Dickey, 2007). An introductory section provided a short illustrated text explaining the process of measuring joint ROM. A quiz, with answers provided on completion, followed the text. This was followed by a series of interactive exercises that simulated the task of measuring various joint motions. For each joint, students activated a video of a moving person, and were required to position a virtual goniometer on the person and read their ROM. This cost AUS$4 000 in photographer and graphic designer costs, and approximately two weeks of one academic staff member’s time.
Students could undertake the interactive exercises at their own pace and could repeat them as often as they wanted as the video would provide a different range of motion for students to measure, each time it was played. Students received immediate feedback on whether they correctly positioned and read the goniometer First, students were asked how to position the model for measurement (Figure 1). Immediate feedback was given on the accuracy of the positioning.
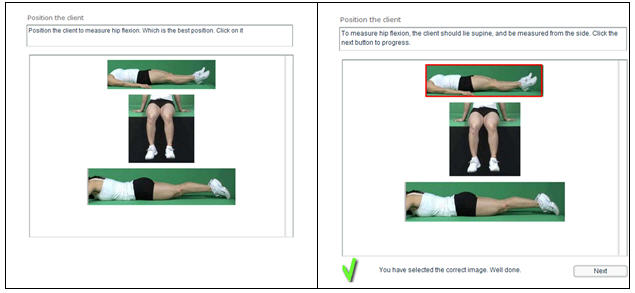
Figure 1: Position the client.
Students were then asked to drag and drop a virtual goniometer onto the picture, in this case, for measuring hip flexion. Then they were prompted to position the axis, the stationary and moveable bars of the goniometer onto the correct surface anatomy sites on the model. When this was done, the model moves and the students were asked to read the goniometer and enter their answer. Again feedback on the accuracy of their response is given immediately.
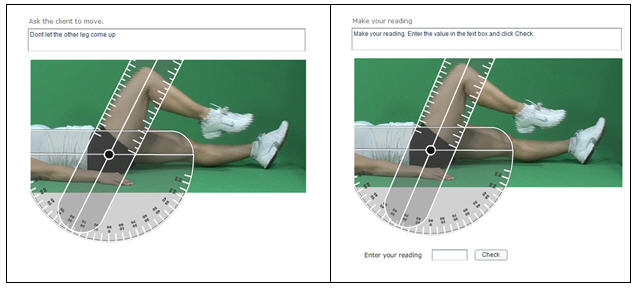
Figure 2. Positioning and reading goniometer
Evaluation
The ROM module was made available to 398 first year students studying human anatomy from the following programs at the University of South Australia: occupational therapy, medical radiation and human movement. All of these students were informed of the module via email and consent was implied by voluntary participation. Students completed the module in their own time at a location suitable to them. Four sections followed an introduction to the ROM module and its purpose, also explaining the study. These four sections were entitled; ‘what is range of motion?’; how do you measure range of motion?’; ‘check your understanding’; ‘interactive range of motion exercises’.
The ROM module was accompanied by an online pre- and post-module questionnaire. The questionnaires were accessible from the anatomy course web site any time during the first six weeks of the study period. The pre-module questionnaire focused on the students’ knowledge and confidence about measuring range of motion (Table I) and the post-module questionnaire additionally explored the students’ experience of the module (Table 2). All student responses were anonymous.
Table 1. Student responses to pre and post joint range of movement module survey.
1. How much do you know about why you measure joint range of motion? |
Pre |
Post |
Nothing at all |
50 |
2 |
Only a little |
109 |
29 |
A good starting knowledge |
38 |
127 |
A lot of understanding for a student |
1 |
40 |
2. What is joint range of motion? |
Pre |
Post |
Measurement of how far a joint moves |
58 |
86 |
Measurement of how straight a joint is |
4 |
7 |
Measurement in degrees of how far a joint moves in one direction |
135 |
224 |
Measurement of how strong a joint is |
0 |
3 |
Overall correct answers |
193 |
310 |
3. Why would you measure joint range of motion? |
Pre |
Post |
To see if your client is really trying |
0 |
0 |
To see if your client has the normal amount of motion normal, or that you would expect in that joint |
77 |
81 |
To be able to record how much motion your client has at the start of treatment, so you both know if s/he improves |
0 |
36 |
To be able to record how much motion your client has so that you can communicate with other people who work with your client |
9 |
112 |
To assess your client’s strength |
4 |
1 |
Overall correct answers |
86 |
229 |
4. A goniometer is .... |
Pre |
Post |
an instrument used by a gynaecologist |
2 |
3 |
a device like a protractor |
93 |
157 |
a device that measures joint motion in degrees |
181 |
220 |
Overall correct answers |
274 |
377 |
5. A goniometer has ...... |
Pre |
Post |
an axis that you place over the joint |
128 |
220 |
a stationary bar that you place over a body part |
73 |
197 |
a moveable bar that you place over a body part |
123 |
189 |
a needle that you insert over the joint |
7 |
3 |
Overall correct answers |
324 |
606 |
N.B. Multiple answers are correct for items two – five; correct answers in italics.
Table 2: Post module survey questions evaluating student perceptions of usefulness and experience of using the joint range of motion module.
Questions and response options |
No of responses |
How clear was the introductory reading? |
Not at all |
0 |
Some parts were clear |
11 |
Most parts were clear |
109 |
It was all clear |
110 |
What I am supposed to learn from this module is . . . . |
not at all clear |
1 |
not clear |
3 |
Clear |
138 |
very clear |
87 |
What did you understand well about the subject matter covered? |
Why you measure range of motion |
204 |
The parts of the goniometer |
37 |
How to position a client |
180 |
How to position the goniometer |
176 |
How to read the goniometer |
114 |
Were you able to follow the exercises? |
very easy to follow |
50 |
easy to follow |
153 |
not that easy to follow |
23 |
difficult to follow |
4 |
very difficult to follow |
0 |
Do you think this online tutorial is relevant to your course? |
very relevant |
71 |
Relevant |
130 |
not that relevant |
26 |
not relevant |
3 |
Once student access to the module had been closed, the pre- and post-module questionnaires were analysed. Questions regarding student knowledge and confidence were compared between pre and post module responses. The data relating to the student experience of the module and its usefulness underwent a content analysis in which common themes were grouped and frequency of occurrence recorded.
Results
Of the 398 potential participants 232 students completed the ROM module and questionnaires, a response rate of 59%. As participation was completely anonymous the questionnaire did not seek data relating to age, gender or discipline group. Not all pre and post questions were answered by every student but nearly all provided short text responses indicating what they liked most and least about the ROM module.
Student knowledge: The pre-module questionnaire indicated 39 students perceived ‘a good starting knowledge’ or ‘a lot of understanding for a student’ in comparison to 167 in the post questionnaire.
Five questions testing student knowledge of ROM were also part of the pre-post questionnaires. Post questionnaire responses showed a 60% increase in correct answers. Interestingly, the question relating to why the student would measure ROM, evidenced the greatest improvement in understanding as an increased number of correct reasons were provided, in comparison to the pre-questionnaire.
Student perceptions of the module: the results of the post-module questionnaire indicated that the 94% of students (n=219) found the module clear and easy to follow. Ninety-seven per cent of students (n= 225) also indicated that they understood what they were expected to learn, and why. In relation to the interactive exercises, 203 students found them easy to follow. Whilst 201 students thought the module was relevant to their course, 29 found the module to lack relevance to their studies.
The option of offering open text responses allowing students to indicate what they liked most about the ROM module, resulted in 216 responses of between one and five lines of text. Analysis of the responses highlights the following themes.
- 61% (n= 141) enjoyed the interactive exercises, particularly the immediate feedback.
- 32% (n= 75) found the introductory information helpful, particularly the layout and the way it was worded.
- 7% (n=17) deemed the accompanying diagrams the best aspect.
- 3% (n=7) appreciated that they could do the module whenever they wanted to.
Two hundred and twenty-three students provided feedback on what they liked least about the module, although of the 223 responses 65 indicated they would not change anything because they found the module to be relevant, clear and easy to follow. However the following aspects where not liked by the remaining respondents.
- 9.5% (n=22) students had trouble loading the interactive exercises onto their computer. Loading time for 1% (n=3) was too long and freezing occurred while they were positioning the goniometer. This caused some students to abandon that exercise.
- 15% (n=38) students found the goniometer was hard to position and a further 12 indicated it was hard to read the goniometer.
- 2% (n=5) students wanted to receive the correct answer in degrees if they read the goniometer wrongly, before they were offered a new exercise.
- 4% (n=9) wanted more information and more interactive exercises.
- 1% (n=3) students said they would prefer to do the exercises in class.
Discussion
There has been a rapid increase in commercially available web-based anatomy learning resources and supports along with course or program specific developments such as the module described in this paper. Moreover, there is discussion regarding the notion of a new generation of students who are comfortable with computers and prefer interactive learning activities (Bennett, Marton & Kervin, 2008). This study indicates that not all students volunteered to engage in interactive web-based learning activities. However, given that engagement in the module was not a requirement of the course, 59% voluntary participation by students indicates that online learning is attractive to students and aids motivation as evidenced in a recent study of German undergraduates (Jastrow & Hollinderbaumer 2004).
The open text responses indicated students enjoyed the interactive element and immediate feedback the ROM module provided, commenting, ‘ the interactive activities are good because they keep you interested while learning the practical approach’, and ‘it was interactive so I was able to get involved in what I was learning’. The timeliness of feedback in relation to learning outcomes is well documented (Biggs & Tang, 2007; Ramsden, 1992). In the ROM module students received an immediate response to each step of the measuring process. Students find such immediate feedback beneficial (Gonzalez, Bernal-Manas & Egea, 2007). The feedback mechanism only allowed for a ‘correct’ or ‘incorrect’ response statement and some students indicated they would prefer to be given the correct answer rather than just an ‘incorrect’ response. Reasons for this preference were not provided by the students, so it is difficult to determine in what way they felt it would support their learning.
There are a number of aspects to the ROM module that require modification and improvements. The module size was problematic for some students and this led to long download times as well as freezing, such issues significantly impacted student motivation to preserve with the module. Impatience with technology is common place in society, with the expectation of quick response times from technology and it is important that web-based learning tools are efficient and responsive to the learner. However, although it is often assumed that students have easy access to computers their internet access and computer software may not be adequate to manage web-based learning modules. The development cost of the ROM module was supported by a teaching and learning grant in terms of the technical support and development. One question unanswered by this study pertained to the ongoing costs of updating and repairing this type of online module. Maintenance and growth of programs would requires graphic design and academic time and skills. The costs in work hours for repairs to make the module more accessible are estimated as AU$750. Expanding the program would require video photography, a model, and further academic and graphic hours, which cost approximately AU$ 4 000 in the first phase of development. In the two years of developing and trialling this module, the university changed its internal online platform, and the graphic program used to create this module changed three times, however the program easily transferred across these software changes.
An additional area of the module that may require improvement is the explanation on how to read the goniometer. Students were required to either ‘click on’ or hover their mouse over the goniometer to view the reading. Although the majority of students did not comment on any difficulties with this, a small number did. This may be the difference between those students who use more complex, interactive or graphic online programmes and those who do not (Bennett, Marton & Kervin, 2008).
The study demonstrates that students were able to answer theory questions regarding ROM more accurately upon completion of the module; however it cannot be determined whether they were better prepared for the practical class or whether they experienced lower levels of anxiety demonstrating the skill to their peers and educator, having practiced the task online. These areas require further investigation.
Understanding the theory behind ROM is the first step in acquiring the ability to measure ROM, having a reusable module can help students learn or revise theory and fact. This study showed that online methods can convey theory and facts about a practical skill. Clinical skills have been taught successfully using online methods. For example, a recent meta-analysis showed that medical students performed better in viva assessments of practical skills if they had been exposed to online simulations of the skill (Cook, Levinson, Garside, Duprais. Erwin and Montori 2008). This study did not assess the actual skill of the students who used the module, nor did it compare with students who did not use the module, but this is the next necessary step
Conclusion
According to Lorenzo & Moore (2002) five aspects of online education should be evaluated: access, student satisfaction, teacher satisfaction, learning effectiveness and cost effectiveness:
- The size of the module needs to be reviewed as some students had difficulty with access.
- Overall, students described satisfaction with the module and pre and post testing demonstrated improved student understanding of ROM.
- Costs associated with maintaining, expanding and repairing the module require investigation and quantification.
- The module requires further evaluation of learning effectiveness of skills, as learning of theoretical background was established.
- Costs associated with maintaining, expanding and repairing the module require investigation and quantification; the cost of creating the module was AUS$4 000.
References
Azevedo, R. (2007) Understanding the complex nature of self-regulatory processes in learning with computer-based learning environments: An introduction. Metacognition Learning, 2, pp. 57-65.
Biggs, J. & Tang, C. (2007) Teaching for Quality Learning at University. 3 rd ed. Berkshire, England; Open University Press.
Brenton, H., Hernandez, J., Bello, F., Strutton, P., Purkayastha, S., Firth, T. & Darzi, A. (2007) Using multimedia and Web3D to enhance anatomy teaching. Computers and Education, 49, pp. 32-53.
Chickering A., & Gamson, Z. (1987) Seven Principles for Good Practice in Undergraduate Education. (special insert) The Wingspread Journal, Vol. 9, No. 2; The Johnson Foundation, Racine:Wisconsin.
Cook, A., Levinson, A., Garside, S., Dupras, D., Erwin, P., & Montori, V. (2008) Internet-Based learning in the Health Professions. Journal of the American Medical Association, vol 300, no 10, pp 1181-1196.
Dickey, M. D. (2005) Engaging by design: How engagement strategies in popular computer and video games can inform instructional design. Educational Technology Research and Development, vol 53, no 2, pp. 67-83.
Hallgren, R. C., Parkhurst, P. E., Monson, C. L., & Crewe, N. M. (2002) An interactive, Web-based tool for learning anatomic landmarks. Academic Medicine Journal, 77, pp. 263–265.
Jastrow, H., & Hollinderbaumer, A. (2004) On the use and value of new media and how medical students assess their effectiveness in learning anatomy. Anatomical Records, 280, pp. 20–29.
Lorenzo, G. & Moore J. (2002) Five pillars of quality online education: The Sloan Consortium Report to the Nation, The Alfred P. Sloan Foundation, viewed 28 August 2009, <http://www.edpath.com/images/SloanCReport.pdf>.
O’Byrne, P.J., Patry, A. & Carnegie, J. A. (2008) The development of interactive online learning tools for the study of anatomy. Medical Teacher, Vol. 30, no. 8, pp.e260-e271.
Patton, Q.M. (1990). Qualitative Evaluation and Research Methods, 2 nd ed. Sage Publications Inc., Newsbury Park, London.
Ramsden, P. (1992) Learning to Teach in Higher Education, London: Routledge.
Scott, T.M . (1993) How we teach anatomy efficiently and effectively. Medical Teacher, Vol. 15, no.1, pp 67-76.